
*Billy is not an actual person, but a composite of several patients Dr. Schwartz has seen over the past several years. Identifying details have been changed to protect their privacy. The treatments and outcomes are real.
Billy is a 7-year-old boy in first grade. I met with his parents for the first session and received a thorough history of Billy’s life. I learned that his mother had no complications during his pregnancy and birth. They shared that he had no known cognitive or social delays. When asked why there were bringing him into therapy at this time, they stated that over the last 4 months Billy was fearful going to sleep at night and he was increasingly anxious separating from his parents during his transitions to school. When asked about significant historical events, his parents stated that when Billy was four his father had been in a car accident and had been in the hospital for about 2 weeks following the accident. Billy and his mother were at home at the time and did not witness the accident but his parents wonder about the impact this accident may have had on Billy.
In order to provide the foundation for successful EMDR treatment for PTSD in children, it is necessary to take the time to develop an in-depth history. I will generally meet with parents first without the child present to inquire significant life events, family systems dynamics, birth and developmental milestones, medical issues, and social and/or cognitive concerns. It is important to for me to understand what are your concerns and goals of therapy. I also want to hear about the strengths of your child so that we can build on what is already working.
My first meetings with Billy introduced him to my office, allowed us to get to know each other, and gave me an opportunity to learn about him through conversation and play. As we continued to get to know each other I shared that this is a place where he can talk about his feelings. To start, we talked about the times and places where he feels calm and safe. Billy brought his stuffed animal in to sessions and we introduced EMDR to his bear. He liked how the “buzzers” felt in his hands. We practiced exercises that Billy can do at home when he feels scared or angry and worked together to find a list of his calming activities for home and school.
As we prepare for EMDR therapy, I work with your child to build a tool kit that helps him or her better manage big emotions. We develop a set of “resources” that your child will use when we get into the “yucky” feelings that can come up when processing a scary event.
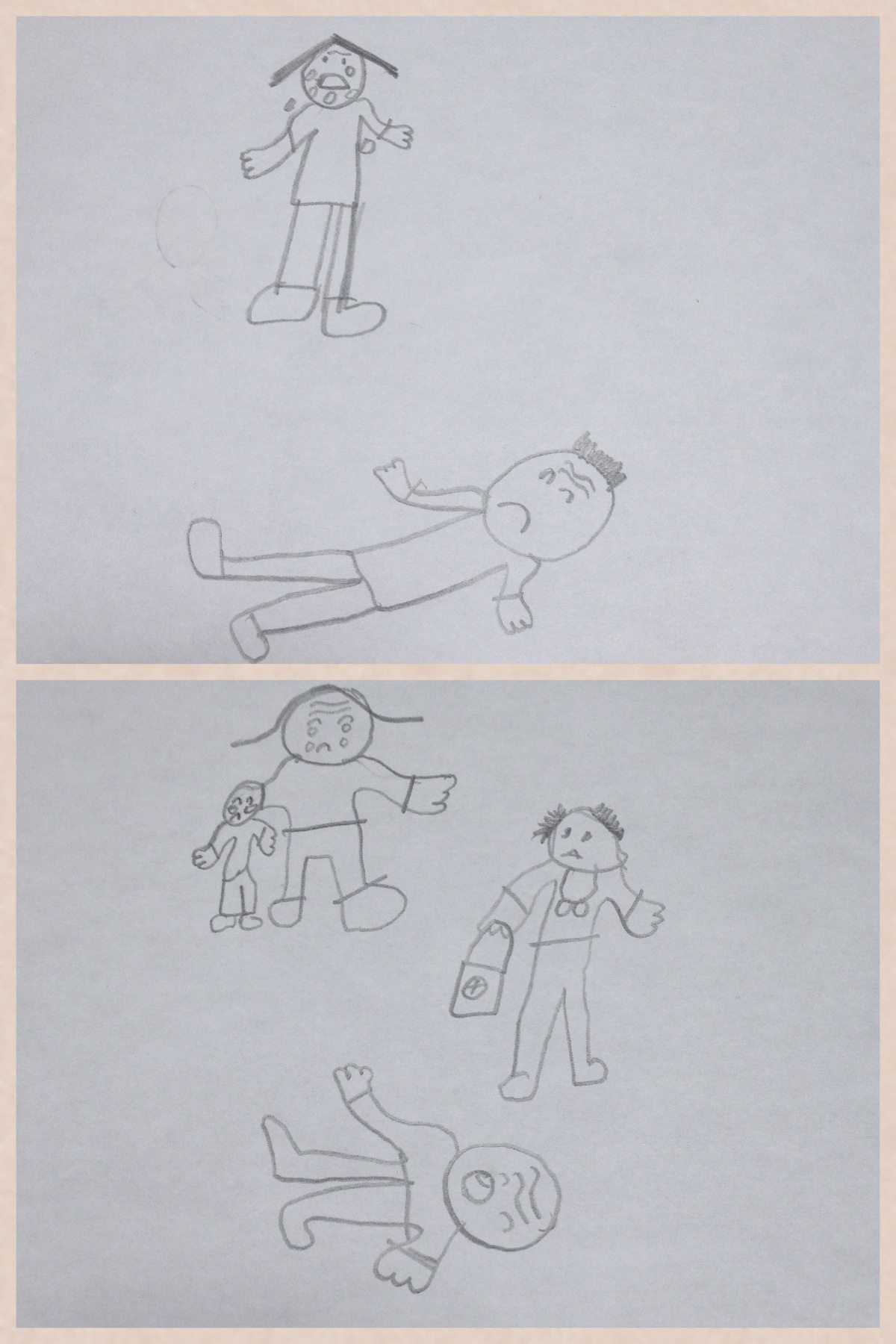
Now that Billy is comfortable with coming into therapy, we start to talk about the “scary” feelings he has when he goes to bed, has nightmares, or leaves for school in the morning. Billy didn’t want to talk about his feelings but preferred to draw them. When asked what he was most afraid of, he shared that he was afraid that something might happen to his parents while he was at school. He drew a picture of his mom crying and his dad lying on the ground. He said it felt very yucky and drew a picture of himself crying too.
At this point in EMDR treatment for PTSD in children I will start with the symptom that is bothering your child. In Billy’s case, we worked with his fearfulness when going to school. While I had not directly brought up the accident that his father had his drawings indicated that his fearfulness may be connected. I shared this information with his parents and encouraged them to talk to him about the event. In the next session, Billy was able to talk about how his dad had a big, scary accident and that he was scared that something like this might happen again.
I asked him to draw a picture now of how he feels when he thinks of dad’s accident.
He drew two cars hitting each other and mom and him crying. Using bilateral buzzers that Billy could hold on to he focused on the “yucky feelings” in his body. Billy squeezed the buzzers tight and scrunched up his face. I reminded him that he can have these big feelings and still be OK. After a little while I gave him a new piece of paper and had him draw how he felt now. This time the drawing changed; his mom and he were hugging and he put a doctor next to his dad. We continued to alternate between buzzer time and drawings, and each time he shared that it didn’t feel so scary anymore. Eventually, he drew a picture of he and his parents hugging and smiling. He was smiling at me too, and got up to do a victory march saying that he felt better.
By using bilateral stimulation, we rhythmically alternate between the two hemispheres of the brain while thinking about a scary event. We know that trauma is primarily stored in both the limbic or mid-brain and in the right hemisphere of the brain. However, we need our entire brain and body to process traumatic events so that the feelings and memories from the past can be resolved. Desensitization of a target can occur in a single session or across multiple sessions but often kids process single event traumas quickly when given the right support.
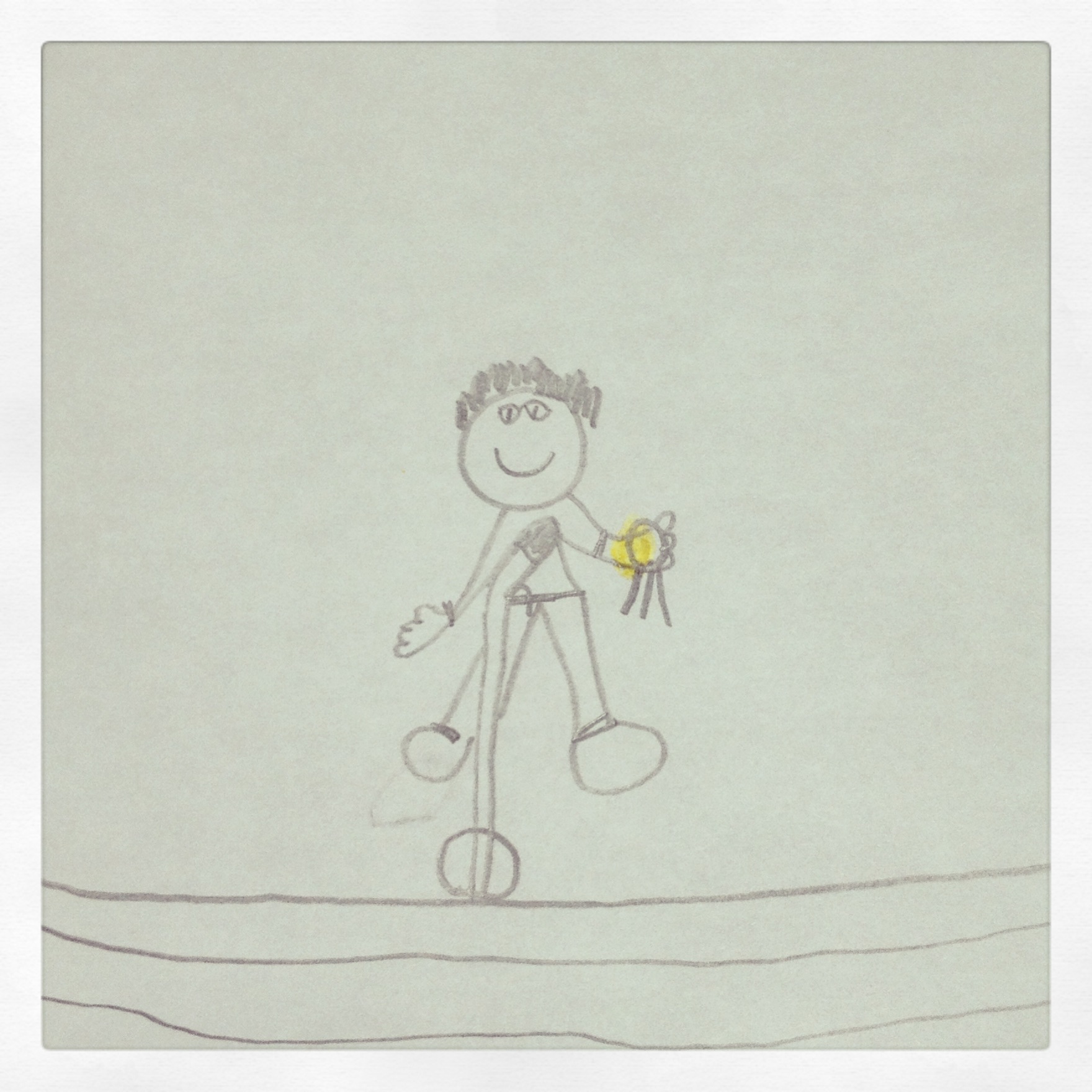
Billy was able to think about the accident and feel better but our work wasn’t done yet. Now, I asked Billy to think about going to school in the morning. At first he said that he was still afraid to leave. When I asked him how he would like to feel he said, I want to feel strong and powerful. I asked him to draw a picture of himself feeling powerful. He drew himself standing on a stage holding a gold medal. I had him imagine his mother dropping him off at school while he looked at his “powerful” picture. We used the buzzers several times until he said the it felt true! We repeated this process with him going to bed at night too.
During the Installation Phase of EMDR treatment for PTSD in Children, I invite a child to strengthen the positive beliefs and feelings and to connect these back to the present life challenges. In Billy’s case, he felt more confident that he could go to school and separate from mom and dad during the day and expressed greater confidence that he could approach them his new found sense of capability.
I gave Billy a flashlight and asked him to imagine that he could shine into the top of his head. I asked him to check inside of his body to see if there is any leftover “yucky” feelings. He said there was just a little bit so we stood up and shook them out. We laughed!
We use the body as a gauge to verify the successful completion of the EMDR process.
Before leaving the session, I invited Billy to think about his calm place and we took a few deep breaths.
Closure is essential to successful treatment in that it allows the challenging work of desensitization to be contained between sessions. When a child still has distress at the end of a session we have a practice to help put them away between sessions. I invite a child to draw a box or we make it with a shoebox so that the “yucky” thoughts, feelings, and memories can stay in a safe place until next time.
In the following session, I asked Billy’s parents and Billy to tell me about his week. I learned that Billy had a much easier time going to school in the morning but he was still scared to go to bed by himself. This let me know where to focus next.
The purpose of re-evaluation allows us to assess the effectiveness of the treatment and address and residual or unresolved feelings.
In Billy’s case EMDR was a very successful treatment of choice. While it is not for every child, EMDR has been well researched and is considered an evidenced based trauma treatment for PTSD in children. Depending on the age and maturity, some children respond better to non-directive play therapy approaches and others respond well to a combination of EMDR and Play Therapy.
Further Reading:

Dr. Arielle Schwartz is a licensed clinical psychologist, wife, and mother in Boulder, CO. She offers trainings for therapists, maintains a private practice, and has passions for the outdoors, yoga, and writing. Dr. Schwartz is the author of The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control and Becoming Whole. She is the developer of Resilience-Informed Therapy which applies research on trauma recovery to form a strength-based, trauma treatment model that includes Eye Movement Desensitization and Reprocessing (EMDR), somatic (body-centered) psychology and time-tested relational psychotherapy. Like Dr. Arielle Schwartz on Facebook, follow her on Linkedin and sign up for email updates to stay up to date with all her posts.